About the Open 3D Model Project
Project 'Open 3D Anatomical Model for Education'

In 2022, a group of anatomists, spearheaded by the department of anatomy and embryology of Leiden University Medical Center (LUMC, Netherlands), in collaboration with anatomists of the department of anatomy of University Medical Center Utrecht (UMCU, Netherlands), of the department of anatomy and embryology of Maastricht University (UM, Netherlands) and of the department of Development and Regeneration of University Leuven, Campus Kulak (KU Leuven, Belgium), with support of the Dutch Anatomical Society ('Nederlandse Anatomen Vereninging' - NAV), obtained a grant from the Dutch Ministry of Education, Culture and Science, to further develop an open-licensed (Creative Commons Attribute ShareAlike CC BY SA) 3D model of human anatomy for usage by medical students and to create a viewer that enables easy online interaction, required for usage by students and teaching staff. Later, anatomists from Amsterdam University Medical Center, location VUmc (Netherlands), from Radboud University Medical Center Nijmegen (Netherlands) and University of Gent (Belgium) also joined the group. The project was named 'Open 3D Anatomical Model for Education'.
History/background
The Open 3D Anatomical Model project built on previous efforts by other groups:
In 2003, a collaboration of several Japanese technical and medical groups (Nat. Inst. of Inform. and Comm. Techn., Kitasato University, Keio University and Tokyo Metropolitan University) had created 3D human voxel models for electromagnetic dosimetry purposes, based on MRI scans of a male and female volunteer, both 22 years old (Nagaoaka 2004).
The above-mentioned male model was built on in the BodyParts3D project. In 2008 it was published by the Database Center for Life Science in Japan (Mitsuhashi 2008). In this project, anatomical structures were identified ('segmented') in the scan, leading to a collection of separate 3D models of 382 body parts. These were released under a Creative Commons ShareAlike Attribute (CC BY SA) license, displayed on the site Anatomography and offered for download. The intent of the project was to create a 'dictionary-type database for anatomy' complementing ontological representation, to serve as a framework for data representation in biomedical research and clinical practice.
Around 2021, a modified version of BodyParts3D was published under the name Z-Anatomy (Kervyn 2022). In this version, structures were added, the meshes simplified ('retopologized') to reduce the file size, vessels and nerves converted into curves, and material properties (colours etc.) and several other features were added (source: personal communication). Several Python scripts where added, to perform specific functions. The Z-anatomy model was also made available under the Creative Commons CC BY SA license. The model is intended to be used in the open source, professional 3D modelling software Blender. Later a version was published that allowed online interaction with the model on the web site Z-Anatomy.
What we did
In the project 'Open 3D Anatomical Model for Education', that started in 2022, we built on the Z-anatomy model and did the following:
1. We remeshed ('retopologized') all structures to remove artificial 'hooked' surface artefacts and to enable smoother modelling by ourselves and future users (Fig 1., compare input file shown in A, B and C, with reworked file, shown in D, E and F.)
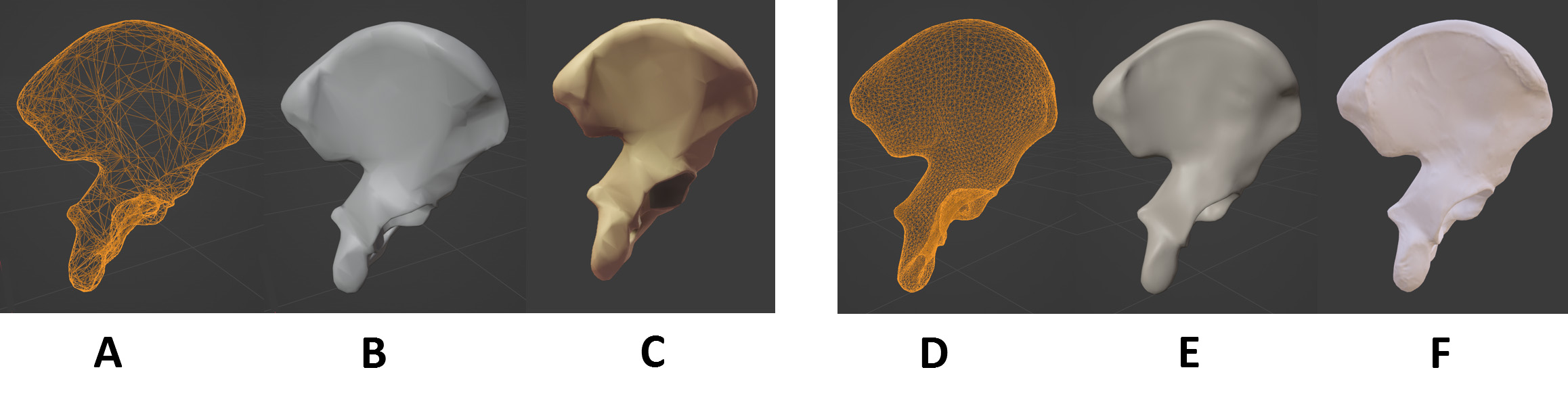
A. Input model mesh,
B. Input model with surface and lighting (in Blender): the mesh causes artificial 'hooked' surfaces that show up due to the lighting and shadows,
C. Input model in online viewer (screenshot taken on 14 July 2025): the lighting accentuates the hooked surfaces.
D. Open3Dmodel retopologized mesh: larger file size than (A) but with more evenly distributed 'points' ('vertices')
E. Open3Dmodel with surface and lighting (in Blender): the more evenly distributed mesh prevents artificially hooked surfaces,
F. Open3Dmodel in online viewer with texture applied (screenshot taken on 14 July 2025): the texture superimposed on the mesh creates a more organic appearance.
2. We reviewed each structure for anatomical correctness and remodelled most structures to correct the anatomy and create a more organic look. Each structure was reviewed by one to three anatomists with expertise in the specific topic. Overall, an estimated 70% of all shapes were changed.
As sources to check against, we used: the anatomist's experience, common anatomical reference works (Moore's, Gray's) and several anatomical atlasses (Netter's, Prometheus, , Pauchet and Dupret). If this provided insufficient information, we searched on Pubmed and Google for scientific publications describing and showing the anatomy or for dissection photo's, or we investigated the issue in the specimens in our dissection labs. For terminology we used Terminologia 1 and 2.
Despite our best efforts, some errors may still be present. We welcome reporting of any mistakes and welcome contributions from anatomists.
An outline of the changes (non-exhaustive listing):
BONES:
- The bones largely kept the outlines of the z-anatomy originals, albeit:
- The bones were modified to give them more organic appearances. This included removing the artificial hooks caused by the original low poly mesh (see above) and modelling a natural appearing surface.
- Some bony features, such as grooves, crests (e.g. making the linea aspera more pronounced), muscle attachment areas, articulation surfaces (e.g. of the sacroliac joint), were adapted.
- The bones of the viscerocranium were extensively remodelled to create an orbit of a more natural appeance and to fit the bones to one another.
- Vertebral facets were better apposed.
- Epiphysial disk lines and fusion lines inherent to the scanned subject's age were made less pronounced (see section 'Developmental features..' below).
- Sesamoid bones of the hand were added.
- Auditory ossicles were newly modelled.
CARTILAGES:
- Articular cartilages (as 3D shapes) were added to all joints, filling the gaps between bones in the articulations.
JOINTS
- Glenohumeral joint: the capsule was given an organic appearance, its ligaments became overlays (see section 'Parts of structures with separate names' below)
- Hip joint: the capsule was given an organic appearance, its ligaments became overlays (see section 'Parts of structures with separate names' below), the zona orbicularis was remodelled
- Symphysis pubicus: the symphysis was extended, the surrounding ligaments completed.
- Sacroiliac joint: the area and surface of the tuberosities of the sacrum and the ilium were adapted and articular cartilage was added to the sacroiliac joint.
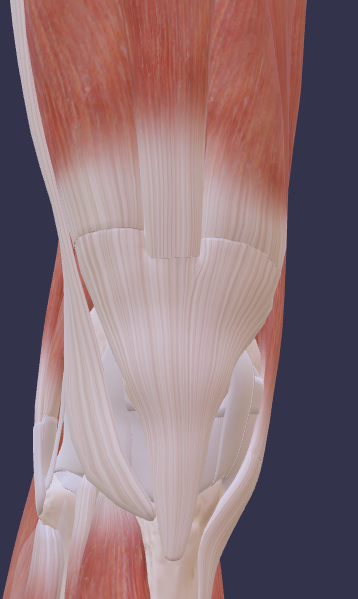
- Knee: the articular capsule (with its oblique and arcuate popliteal ligaments), the cruciate ligaments and the synovia were extensively remodelled.
- Intervertebral disks: the anuli fibrosi and nuclei pulposi were remodelled.
BURSAE AND SYNOVIAE
- Bursae were newly modelled.
- The synovial sheaths in the upper and lower limb were extensively remodelled, increasing anatomical correctness as 'balloon'-like structures with outer and inner layers and a lumen, wrapped around the tendons, with a slit where the 'wrapped' ends meet.
MUSCLES, TENDONS, APONEUROSES, INVESTING FASCIA
- The muscles largely kept the outlines of the original z-anatomy originals, albeit:
- Tendons or aponeuroses were often added or adapted.
- (Mostly small) shape changes were made and/or attachments of several muscles were adapted.
- Separate common tendons were created for muscles with multiple heads joining in a joint tendon and for multiple muscles joining in a joint tendon (see section 'Joint tendons' below),
- Some small muscles were added.
- The muscles and tendons were given a natural appearance with textures.
A (non-exhaustive) listing of muscles with changes:
- Scaleni (ant/mid/post) (adapted attachments and/or shape)
- Levator glandulae thyroideae (added)
Back muscles:
- Semispinales (capitis/cervicis/thoracis) (adapted attachments, extended)
- Thoracolumbar fascia (extended to cover erector spinae muscles from thorax to sacrum)
Thoracic muscles:
- 1st Internal and innermost intercostal muscles (added), subcostals (added), transverse thoracic (added tendon parts)
- Diaphragm (adapted shape) - central tendon, sternocostal triangle, lumbocostal triangle, arcuate ligaments (median, medial, lateral), pillars of right crus, suspensory muscle/ligament of duodenum ('Treitz ligament') (all added)
Axio-appendicular muscles:
- Pectoralis major, serratus anterior, trapezius, latissimus dorsi, subclavius (small changes to shape and/or attachments)
Upper extremity muscles:
- Deltoid, teres minor, teres major, supraspinatus, infraspinatus, subscapularis, biceps brachii, brachialis, extensor carpi ulnaris, opponens pollicis, extensor digitorum, extensor indicis, extensor digiti minimi, flexor carpi ulnaris, flexor carpi radialis, flexor pollicis brevis, flexor pollicis longus, abductor pollicis brevis, palmar interossei, dorsal interossei (small changes to shape and/or attachments)
- Bicipital aponeurosis, palmaris brevis (added)
Abdominal wall muscles:
- Internal abdominal oblique, transversus abominis, quadratus lumborum (adapted shape and/or attachments)
- Structures forming the inguinal canal, inguinal ligament, anulus internus/externus (remodelled or added, to form the inguinal canal)
- Cremaster muscle, aponeuroses of abdominal wall muscles and rectus sheath (added)
Pelvis & perineum muscles:
- Iliococcygeus, pubocococcygeus, puborectalis, coccygeus (adapted shape)
- External anal sphincter (remodelled into deep, superficial and subcutaneous parts)
- Superficial transverse perineal, ischiocavernosus, bulbospongiosus (added)
Lower extremity muscles:
- Gluteus maximus, gluteus medius, psoas major, psoas minor, pectineus, piriformis, obturator internus, obturator externus, adductor magnus, adductor minimus, sartorius, gracilis, rectus femoris, semimembranosus, pes anserinus, popliteus, plantaris, tibialis anterior, tibialis posterior, fibularis longus, fibularis brevis, fibularis tertius, gastrocnemius, soleus, flexor digitorum longus, flexor digitorum brevis, flexor hallucis brevis, flexor digiti minimi, extensor digitorum brevis, extensor hallucis brevis, opponens digiti minimi, quadratus plantae, lumbricals, abductor hallucis, adductor hallucis (small changes to shape and/or attachments)
- Articularis genus (added)
LIGAMENTS
- Where capsules have parts with specific 'ligament' names, we used an 'overlay' technique, described below in section 'Parts of structures with separate names'. This concerns for instance the capsules of the shoulder, hip and the knee joints. Also fibre directions in the capsules were modelled.
- The same overlay technique was applied to ligaments with named parts, e.g. the trapezoid and conoid ligaments which are parts of the coraco-clavicular ligament., and to local thickenings within fascial sheets that are indicated as 'ligaments', such as the cardinal ligament or the recto-uterine (sacrouterine) ligament in the pelvic fascia.
- Many ligaments were (extensively) remodelled: e.g. ligaments of the back (e.g. nuchal ligament, ligamenta flava, supraspinous ligament), ligaments of the pectoral girdle (coracohumeral lig., coraco-acromial lig., superior, middle, inferior glenohumeral ligg., transverse humeral ligament), and several other ligaments of the upper and lower limb and of the pelvis (e.g. the sacrospinal and sacrotuberal ligaments)
- Several ligaments were added: e.g. flexor retinaculum (transverse carpal ligament) of the wrist, fibrous tendon sheaths of the digits, anular parts of fibrous sheaths of the fingers, lateral bands of the fingers, extensor hoods of the digits, oblique ligament of 1st finger, interclavicular ligament, facet joint capsules, phrenicooesophageal ligament, median umbilical lig., anococcygeal lig., puboprostatic ligaments, suspensory ligament of the penis.
- Several fascias in the pelvis were added or remodelled: obturator fascia, perineal membrane, pudendal canal (Alcock's), Buck's fascia, Dartos/Colles' fascia, Gallaudet's fascia, tunica albuginea, internal and external spermatic fasciae.
- The capsules and ligaments were given a natural appearance with textures.
BLOOD VESSELS
- All blood vessels in the upper and lower limb were newly modelled.
NERVES
- All nerves in the upper and lower limb were newly modelled.
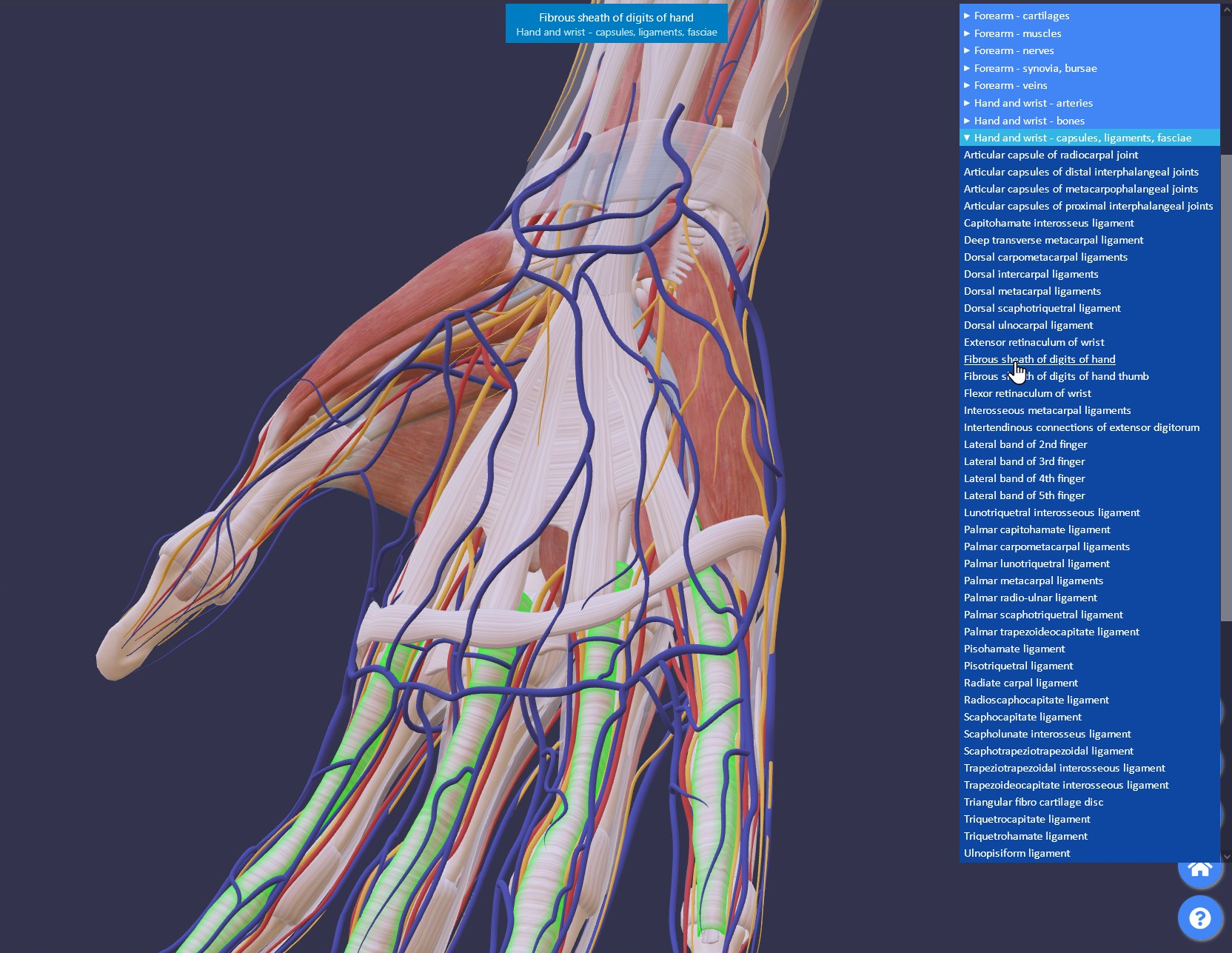
3.We developed a web viewer (see Fig. 2) that allows easy navigation of the models (rotating, zoom, pan), hiding and unhiding structures on individual and group level, and that displays the name of the selected structure. By adding a tag to the URL an export functionality becomes available that exports a list of currently visible structures. This functionality can be used by staff who want to have a sub model created with a specific subset of structures. The viewer is offered under GPL3 license on GitHub.
Canonical anatomy
Anatomy may vary largely between different individuals. In atlases, sizes, configurations, etc. of depicted structures also may vary. For the Open3Dmodel we aimed at creating 'canonical' adult anatomy. As a criterion to judge the correctness of a structure, the anatomist judged whether it was within the range of appearances known to the anatomist from their own experience or as described in literature.
Developmental features: epiphysial disks and fusion lines
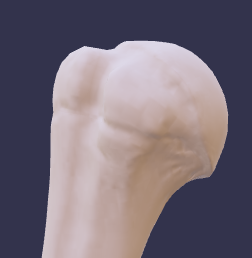
One issue arose when aiming at creation of adult anatomy models: the scanned subject, on whom the model is based, was a 22-year-old person. This implied that some epiphysial disks or fusion lines were not yet fully closed, as would be the case with an older adult. However, we felt that it might be useful to show these epiphysial lines, especially as in clinical practice they may be accidentally mistaken for a fracture. We took the 'middle way' in this dilemma: we made such epiphyseal lines or fusion lines less pronounced, but left them visible as shallow lines, see Figs. 3 and 4 for examples.

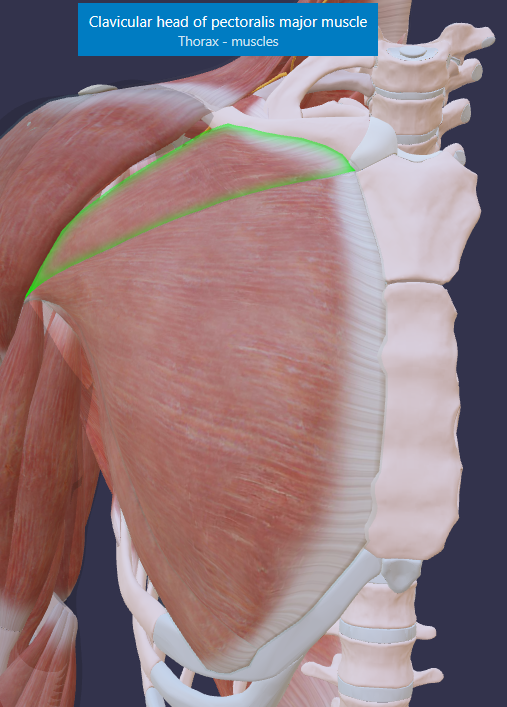
Parts of structures with separate names
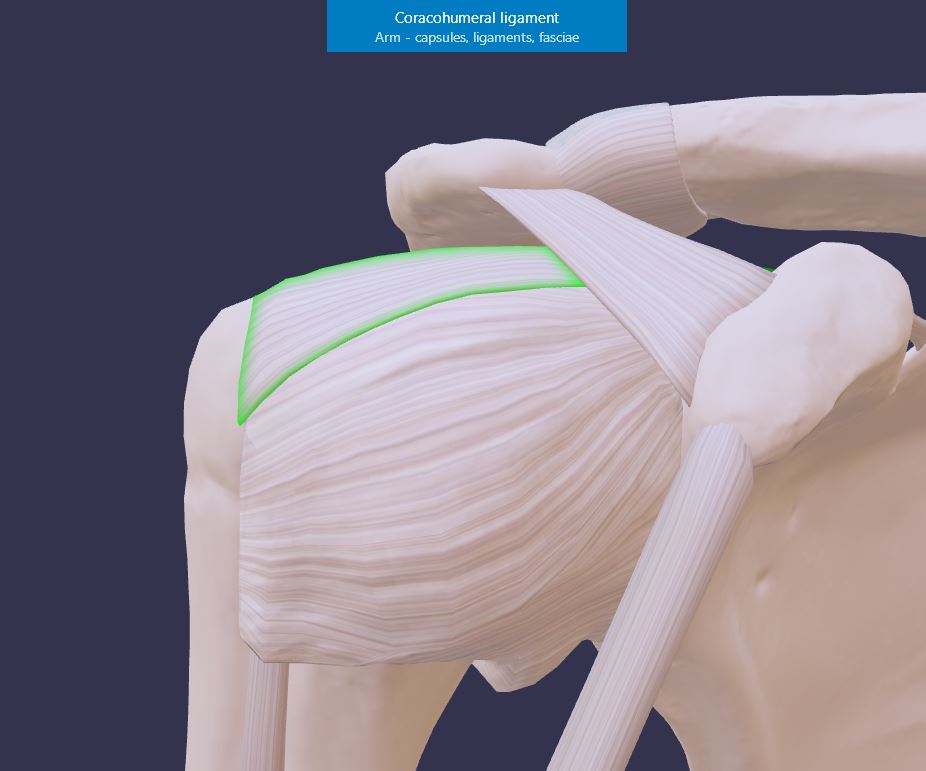
In many cases, parts of structures have been given separate names. For instance, in capsules or fascial sheets, parts are often recognized that are thicker or that appear denser when pull is exerted to them. Such denser parts are often referred to as specific 'ligaments', whereas they in fact are only thickened parts of continuous capsules/sheets. Hence, there is an anatomical reality (the capsules or fascial sheaths are one, continuous entity) and a didactical need to be able to identify the parts that have received specific names.
In a 3D model, to show these specific parts, one can create separate objects for them, which can be individually shown or hidden. One could thus split up a capsule into several 'ligaments' and unnamed parts in between. However, this would give the false impression that these capsules are indeed fragmented structures. Alternatively, one could create both the capsules and ligaments as separate objects, where clicking the 'ligament objects' would satisfy the didactic naming need, but this would wrongly give the impression that the 'ligaments' are separate structures besides the capsules. Moreover, all those approaches mostly results in an unnatural appearance.
To solve this dilemma, we chose 1) to follow the anatomical reality and create the capsules and fascial sheaths as continuous structures and 2) to use transparent, green glow, 'overlays' on top of the main structure, that can be hidden or shown, to indicate where the specific 'ligaments' in the capsule lie. Fig. 5 shows an example of this.
The same 'overlay' technique was used to indicate parts of muscles, for instance, parts with specific attachments (see Fig. 6 for an example), used in ligaments with named parts (see Fig. 7 for an example), and in fascia sheets with named ligamentous parts (no example). Usually, the overlays are initially hidden, to avoid having to first remove several overlays before accessing the name of the main structure or being able to hide it. The overlays/parts can be found and shown via the menu listing of structures.

Joint tendons
Muscles with multiple heads or different muscles may converge in a joint tendon, with the tendon fibres interweaving.
However, in a 3D model interweaving objects are undesirable. In such cases, the modeller sometimes attaches one main tendon to the bone, while the other tendons taper out on the side of this main tendon. The disadvantage of this approach is that if the main muscle/tendon is hidden, the tendons that insert on it, seem to end somewhere 'in mid air'. Moreover, such tapered free endings appear unnatural. Another solution would be to join all heads or all contributing muscles into one single object. This would create a natural appearance, but also would sacrifice the possibility of hiding or showing the individual muscle heads or muscles.
Therefore we chose a third solution: namely creating a separate object for the terminal joint tendon part and connecting that with distinct sharp cuts to the contributing multiple heads/muscles, clearly visualising that these heads/muscles all connect to the joint ending, while the heads/muscles could still be hidden or shown individually. Fig. 8 shows an example.
Status
The Open3Dmodel project is a work of progress. In July 2025, we published the first results. By then we had approximately finished modelling:
- the skeleton
- the muscles of the trunk and extremities
- all structures of the upper and lower limb
- the structures of the male pelvis
During Q3 and Q4 of 2025 and Q1 and Q2 of 2026 we plan to work on the internal structures, the non-skeletal structures in the head and neck, as well as the female organs.
Additionally, the creation of derivative learning materials (see below) is an ongoing process, with materials being added gradually.
With a project of this scale, it is unavoidable that errors may go unnoticed. We encourage anyone - whether anatomists, students, health care practitioners or other experts - to report encountered errors to us. We will acknowledge and credit those who submit corrections that enhance the anatomical accuracy of the model.
Derivative learning material
Based on the 3D model, sub models, videos, presentations and 2D images for educational use are made. They can be found open3Dmodel-learn page.
Create and develop
Teachers who would like to create sub-models with specific selections of structures can make such selections, using so-called Selection models.
3D modellers and/or anatomists who want to further develop the model, can do so using the source files.
The creation and distribution of any derivative materials from the open3Dmodel should comply with the Creative Commons license's requirements stated with the material.
The selection models, source files and manuals can be found on the open3Dmodel-create page.
One can create and publish one's own derivative models and educational material, but we cordially invite departments of anatomy or individual anatomists, who would like to participate and contribute to the further development of the model and its educational derivatives to join the current group to bundle forces. To contact us, please see the open3Dmodel-contact page.
Credits
The project-team and all contributors are listed on the open3Dmodel-credit page.
Bibliography
- Anatomography http://lifesciencedb.jp/bp3d/
- Kervyn G. 2022. The First Open Source 3d Atlas of Human Anatomy. Acta Scientific Anatomy 1.4 (2022): 13-15. https://actascientific.com/ASAT/pdf/ASAT-01-0022.pdf
- Mitsuhashi N et al. 2008. BodyParts3D - 3D structure database for anatomical concepts. Nucl Acids Res, 2009, Vol. 37 https://pubmed.ncbi.nlm.nih.gov/18835852/ , https://dbarchive.biosciencedbc.jp/en/bodyparts3d/desc
- Nagaoaka et al. 2004. Development of realistic high-resolution whole-body voxel models of Japanese adult males and females of average height and weight, and application of models to radio-frequency electromagnetic-field dosimetry 10.1088/0031-9155/49/1/001
- Moore's Clinically Oriented Anatomy 7th and 8th ed.
- Gray's Anatomy 40st and 41st ed.
- Netter's Atlas of human anatomy
- Prometheus Thieme Atlas of Anatomy 1st ed.
- Sobotta Atlas of Human Anatomy 15th ed.
- Pauchet and Dupret L'Anatomie en Poche, 1926
- Terminologia Anatomica 1, FCAT, IFAA, Thieme. 1998
- Terminologia Anatomica 2, https://ta2viewer.openanatomy.org/
- 9190 reads